The thyroid is an endocrine gland located at the base of the neck, and surgery is often necessary following the occurrence of endocrine disorders or tumor nodules.
This is a delicate surgery and not without consequences and risks that must be carefully analyzed before considering an intervention.
Thyroidectomy consists of the partial or total removal of the thyroid gland, an endocrine gland (which produces hormones) located in the antero-inferior and medial part of the neck.
.JPG)
.JPG)
mass of the base of the neck
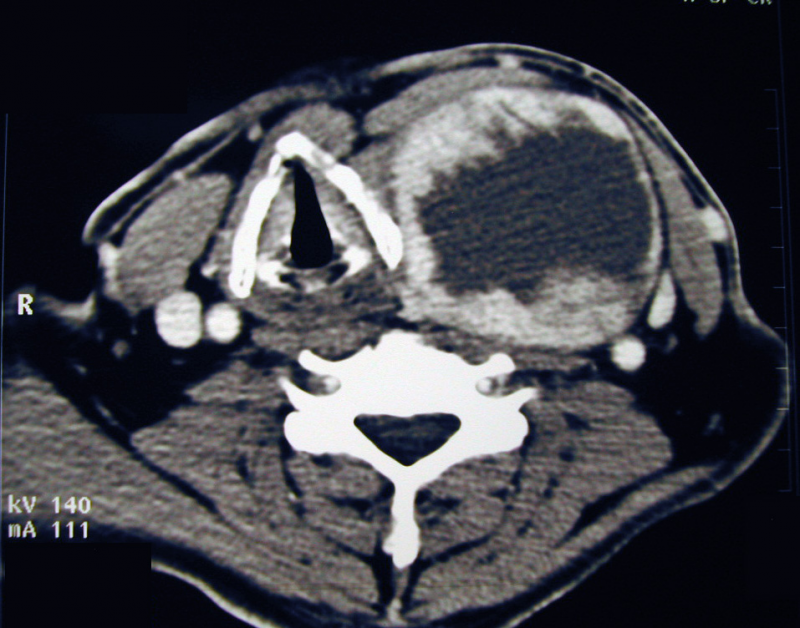 large thyroid cyst
large thyroid cyst
PURPOSE OF THE INTERVENTION
This intervention can have several goals:
• specify the nature of one or more nodules detected in the thyroid.
• removing all or part of the gland due to malfunction, not controlled by medical treatment.
• Remove all or part of the gland due to its size and the risk of compression of surrounding structures
• to prevent the occurrence of cancer in cases of proven genetic risk (family history of multiple endocrine neoplasia)
PERFORMANCE OF THE INTERVENTION
This procedure is usually performed under general anesthesia. The skin incision is horizontal, located in the lower, mid-neck area, ideally within a natural skin crease. The length of the incision will be determined by the type of procedure and the size of the gland (goiter).
Depending on the proposed intervention, the following will be carried out:
• the removal of an isolated nodule (enucleoresis),
• a lobo-isthmectomy, namely the removal of half of your thyroid gland,
• a subtotal thyroidectomy,
• a total thyroidectomy.
A microscopic tissue analysis of the nodule(s) may be requested during the procedure (frozen section examination, with immediate analysis but a non-definitive result and not 100% reliable) to determine the nature of the tumor and adjust the extent of the surgery. In the case of a malignant tumor, a total thyroidectomy is standard practice and will be combined with the removal of lymph nodes located in the neck region and along the trachea, depending on the initial assessment. This procedure will require enlarging the surgical incision if the lateral lymph nodes in your neck are removed. One or more drains will usually be inserted depending on the extent of the surgery.
The hospital stay is 2 days, necessary for the removal of the drain; the pain is mild, mainly due to the prolonged position of the head in extension following the procedure.
An intradermal suture is removed after 8 days
SURGICAL RISKS
First and foremost, the hematoma in the neck may require further intervention to evacuate the hematoma, which compresses the trachea and can impede breathing.
In the case of a total thyroidectomy, cramps and tingling in the hands or feet may occur, related to parathyroid gland dysfunction due to a drop in blood calcium levels. These symptoms are usually temporary and require medical treatment.
The main risk remains trauma to the recurrent laryngeal nerve (responsible for vocal cord mobility), which can cause voice disorders that are most often transient and may require temporary rehabilitation. These voice disorders can be accompanied by swallowing difficulties and shortness of breath during exertion. Respiratory problems can be serious and may require ventilatory support, or even a tracheotomy or laryngeal surgery. It is also important to mention the rare complications of tracheal necrosis following total thyroidectomy and lymphatic leakage in cases of associated lymph node dissection.
SURGICAL CONSEQUENCES:.JPG)
Total or near-total removal of the thyroid gland necessitates lifelong hormone replacement therapy to compensate for the lack of hormone production. In the case of partial thyroid removal, thyroid hormone secretion should be monitored by blood tests performed some time after the procedure (depending on the results, hormone therapy may be prescribed).
The scar may develop adhesions or become thickened.
