Related procedure: Treatment of nasal obstruction or sinusitis
Some nasal obstructions are not solely due to a deviated septum; they can be secondary to a
increased volume of the inferior turbinates or a weakness of the cutaneous or cartilaginous structure of the nasal tip.
TURBINOPLASTY OR PLASTIC REMOVAL OF THE INFERIOR TURBINE
A thorough examination of nasal function before considering rhinoplasty or septoplasty should also look for abnormal enlargement of the inferior turbinates due to simple chronic inflammation or associated allergic rhinitis. Hypertrophy of the inferior turbinate on the side opposite the deviated septum is often present.
It is then necessary to determine whether a reduction in the volume of the inferior turbinates is indicated. Complete turbinectomy, which is blamed for causing empty nose syndrome , is no longer performed. Instead, turbinoplasty is used to reduce the volume of the inferior turbinates using radiofrequency ablation or a flexible fiber laser, performed simultaneously with the surgical procedure. This combined procedure is simple and quick, allowing for the reduction of excessive volume of the inferior turbinate mucosa while preserving its function. This intervention is performed endoscopically, that is, using microsurgery with a camera and screen system.
 |
 |
||
|
Right wall deviations
|
with excess volume of the cornea lower left |
 |
 |
||
|
|
Right wall deviations without excess volume of the cornea lower left |
large lower right turbinate |
TREATMENT OF NASAL VALVE WEAKNESS
In some patients, nasal obstruction is not due to a deviated septum or inferior turbinate hypertrophy, but rather to a weakness in the skin or cartilage structure of the nasal tip.
This is especially true for patients who have already undergone rhinoplasty with cartilage sacrifice, which alters the structure of the nasal tip; sometimes it involves a patient with a thick tip and a bulbous tip.
In this case, appropriate surgery using cartilage grafts is necessary, in the area of spreader-grafts which widen the lower part of the nasal pyramid, sometimes accessory procedures such as plasty of the piriform openings may be justified.



Nasal valve weakness post-rhinoplasty, acquired (post-operative) weakness
.JPG)
.JPG)
Constitutional weakness of the nasal valve
Nasal Valve Intervention with Graft Spreader Placement
|
|
 |
||
| Cartilage growth on the nasal septum | projection of cartilage arrangement |

|
|
 |
 |
|
| Grafts in place | closure of the external route |
TREATMENT OF ASSOCIATED SINUSITIS
These conditions can coexist with respiratory problems, particularly chronic sinusitis or a tendency towards recurrent acute sinusitis. In such cases, they can be treated simultaneously with a meatotomy, which is an enlargement of the natural opening of the maxillary sinus into the nasal cavity. Only severe sinusitis or nasal polyps warrant a two-stage surgical procedure.
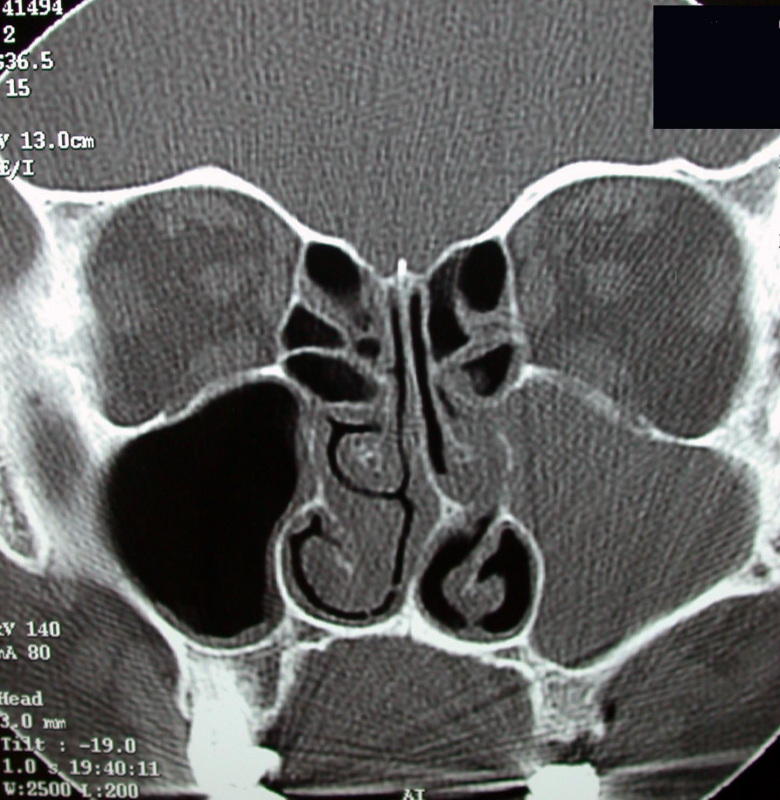
All these procedures involve endoscopic microsurgery, leaving no visible scar and without additional external swelling. A pre-operative CT scan is an essential radiological element before this type of procedure.
|
|
|
|
| Left maxillary sinusitis | foreign body in the right sinus meatus |
Anatomical anomaly called concha bullosa of the left middle turbinate |