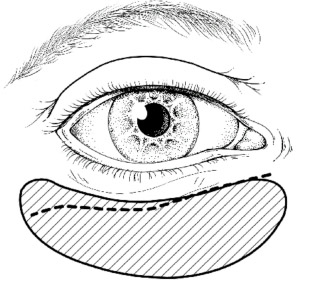
Ultimately, the ptosis and hyperlaxity of the lower eyelid will be corrected by reinforcing it with conchal cartilage, deposited through a subtarsal incision between the septum and the orbicularis oculi muscle (Figure 1). This technique corrects scleral show (abnormal gap between the lower edge of the iris and the free edge of the lower eyelid when viewed from the front), significantly reduces tearing and eyelid eversion, and improves eyelid closure. (1)
Figure 1:
The lower eyelid is articulated by conchal cartilage
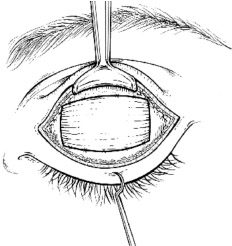
The retraction of the upper eyelid will be compensated for by lengthening the levator muscle: this muscle is dissected and then sectioned. A fascia lata interposition graft (taken from the thigh) is inserted, its width being twice the length of the desired eyelid lengthening (Figure 2). This technique has replaced the use of gold plates: these plates invariably end up protruding, leaving a fibrous and hypertrophied levator muscle that is extremely difficult to correct later. Botulinum toxin injected under electromyographic guidance is an alternative to this surgical procedure, but its use is delicate: its diffusion to the lacrimal gland causes detrimental dry eye in this context. Diplopia is also possible due to diffusion to the superior rectus muscle.
Figure 2:
Lengthening of the levator palpebrae superioris muscle
In elderly patients for whom a coronal approach would be too invasive, eyebrow ptosis can be corrected by a slanted supraorbital skin resection. Alternatively, the coronal approach used for accessing the temporalis muscle (see below) allows for a mask lift (2) and an external canthopexy, which yield very good results in this indication.
All of these procedures must always be accompanied by close ophthalmological monitoring.
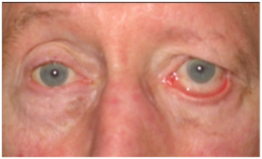
Severe form of facial paralysis
Before and after
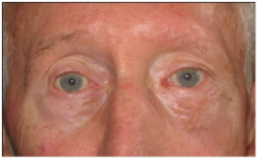

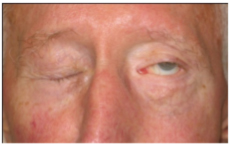
Rehabilitation of paralyzed eyelids
Before and after




